
To the Editor:
Brugada syndrome, an entity described in 1992,1 is characterized by episodes of syncope or unexpected sudden death in patients with a structurally normal heart, and a characteristic electrocardiogram consisting of a right bundle-branch block (RBBB) pattern and ST segment elevation in the unipolar precordial V1 through V3 leads. The electrocardiographic pattern may be present, intermittent, or occult (only demonstrable with a test done with flecainide, procainamide, or ajmaline). The arrhythmic event can occur at rest, triggered by stress, or with no apparent relationship, with variations in the autonomic nervous system. There are 3 types: type 1, which presents coved ST-segment elevation ≥2 mm, followed by negative T-wave; type 2, with saddleback ST segment elevation and J point ≥2 mm, followed by positive T-wave; and type 3, with ST segment elevation and J point <1 mm and variable morphology (coved or saddleback).2
We describe a patient with the characteristic ECG features of Brugada syndrome who was found to have sustained monomorphic ventricular tachycardia (SMVT) during exercise testing, an observation for which we found no references in the scientific literature.
Exercise testing is a procedure used for the diagnostic and prognostic assessment of patients with ischemic heart disease that is also used in other subjects, both healthy and ill, with nonischemic heart disease.3
A 38-year-old man with no personal or family history of interest was referred for exercise testing due to episodes of chest pain. He was not receiving any therapy.
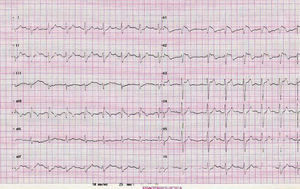
The baseline electrocardiogram (ECG) was performed without medication and showed the characteristic image of type 1 Brugada syndrome, with RBBB and ST segment elevation in V1, V2, and V3 (Figure 1).

Figure 1. Baseline electrocardiogram shows the classic pattern of Brugada syndrome.
The exercise test was done using the Bruce protocol, with 10:08 minutes of exercise. After 1 minute of recovery, the patient presented SMVT with RBBB morphology at a rate of 180 bpm that lasted 40 s but showed no hemodynamic repercussions (Figure 2). He did not present chest pain at any time during the test, which was clinically and electrically negative for ischemia.

Figure. 2. Onset of ventricular tachycardia at minute 1:14 of recovery (left). Sustained ventricular tachycardia (right).
The patient was admitted to our hospital, where transthoracic echocardiography showed normal systolic function, with no regional contractility abnormalities, or other pathological findings of interest. Left catheterization for coronary angiography and ventriculography yielded normal results.
Electrophysiological study was later performed, in which 3 extrastimuli were applied to the apex of the right ventricle, but only nonsustained ventricular tachycardia was achieved.
An implantable cardioverter defibrillator was indicated, based on the possibility of malignant arrhythmia, which had been documented with the stress test.
Among the 3 siblings, only 1 presented pathological baseline ECG findings (type 2); he has a son with a type 1 ECG pattern. An EEF study was performed, but arrhythmia was not induced. At the time of writing, after more than 12 months of follow-up, no arrhythmic event has been observed and the baseline ECG is always similar to the previous one.
The patient presented no chest pain during the exercise test, not even during the episode of sustained monomorphic ventricular tachycardia. Therefore, we must presume that the clinical symptoms are not related to the tachycardia. Furthermore, the patient had not previously reported the presence of palpitations and syncopal episodes. An ischemic etiology of the tachycardia was ruled out by catheterization.
The malignant ventricular arrhythmia documented in our case presented during early recovery from the exercise test, immediately after maximum effort, when the sympathetic stimulus produced by exercise starts to diminish. Vagal tone is greater at this time and may have been the cause of the arrhythmia. An interesting aspect of this case is the negative EEF results. These 2 points are important, because the electrophysiological study, a diagnostic test of proven usefulness, was negative, whereas a nonroutine test for this condition triggered arrhythmia.
It is worth noting that our patient SMVT, although sustained polymorphic ventricular tachycardia is much more common in this syndrome. It is also interesting that the tachycardia presented RBBB morphology, which is evidence of left ventricular origin, making this an even more curious case. In our opinion, this isolated finding does not provide a basis for recommending routine use of exercise testing for Brugada syndrome in clinical practice, although there may be a group of patients in whom recovery after strenuous exercise triggers arrhythmia, making it advisable to conduct prospective studies to determine whether the test should be routinely done among such patients.