
To the Editor,
Poor lead positioning of implantable electronic cardiac devices is rare and discovered incidentally on occasion, but can have serious complications.1 Dislodgement of correctly positioned leads is common, however, and can be a significant source of clinical complications for patients with these devices. Lead dislodgement may be an incidental, asymptomatic finding in certain patients, while in others it can cause a wide range of clinical problems. These include extracardiac stimulation, inappropriate therapies by automatic defibrillators, syncope, and heart failure due to loss of cardiac resynchronization in patients with biventricular pacing, possibly leading to death from asystole in patients completely dependent on pacing..
Leaving aside injuries and iatrogenic conditions, several syndromes of lead macro-dislodgement have been described and cover the usual causes of lead dislodgement, namely, twiddler, reel, and ratchet syndromes.2, 3, 4 Although the problem is relevant, the terminology is confusing, perhaps because these terms were originally taken from individual case reports in the literature. Identical cases have been defined and classified differently by the authors and, conversely, different cases have been classified as identical. Some cases initially described as twiddler syndrome are actually forms of reel syndrome, and some cases described as either of these entities are actually cases of ratchet syndrome.5, 6 Therefore, it would be appropriate to provide precise definitions for each of the potential mechanisms, in order to enhance our understanding of the mechanisms involved in each patient and to identify predictors of the problem, their consequences, and the frequency of actual presentation of each one..
Below we present a proposal for the precise definition and classification of these lead macro-dislodgement syndromes (Figure 1):.

Figure 1. Mechanisms involved in lead macro-dislodgement of implantable devices. A, normal. B, twiddler syndrome. C, reel syndrome. D, ratchet syndrome.
Twiddler syndrome: Twiddler syndrome can be defined as lead retraction and dislodgement due to device generator rotation over the axis defined by the lead. Although external manipulation by the patient may make it easier for this to occur, it is not a necessary condition. As the generator rotates, the lead twists over itself, giving it a characteristic and definitive appearance (Figure 2)..

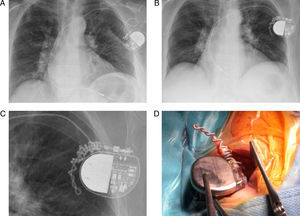
Figure 2. Example of twiddler syndrome in a 68-year-old patient who presented macro-dislodgement of the ventricular lead of a pacemaker implanted 2 months previously for atrial fibrillation with significant pauses. A, posteroanterior chest radiograph showing a normal lead position. B, posteroanterior chest radiograph showing lead macro-dislodgement and winding of the proximal portion over the long axis, due to generator rotation over the horizontal axis. C, detailed view of the proximal portion and generator in the radiograph. D, detailed view of the surgical revision of the system.
Reel syndrome: Reel syndrome can be defined as lead retraction and dislodgement due to generator rotation over its sagittal axis, which causes lead reeling above or below the generator. Because of the mechanism involved in both twiddler and reel syndrome, all leads would be affected to some extent, in case of several leads..
Ratchet syndrome: Ratchet syndrome can be defined as lead retraction and dislodgement due to progressive lead displacement through its fixation parts or protector sleeves, facilitated by movements of the ipsilateral arm and due to incomplete lead fixation to the protector sleeve, but without generator rotation over any of its axes. In this case, the problem could involve all system leads in a patient or, more commonly, only one of the leads, with all others in normal position; this is a key finding for identifying ratchet syndrome and distinguishing it from the other 2 lead macro-dislodgement syndromes..
Prior to surgical revision of the system in the case of lead dislodgement, simple visualization of the lead(s) and radiographic visualization of the generator position, along with a comparison to the original implant position, will provide an approximate identification of the mechanism involved. For cases in which the evidence is not definitive, either because the system uses only 1 lead and there are no signs of any mechanism (eg, twisting) or because the generator is in its normal position and there are no lead abnormalities, it would be preferable to use the term “lead macro-dislodgement” alone..
We believe that the classification and management of the proposed definitions may be helpful to the clinician and to the physician implanting the device and would allow better characterization of this rather common complication in patients with implantable electronic cardiac devices..
.
Corresponding author: maapalomares@secardiologia.es