

We present the case of a 24-year-old male, asymptomatic, examined at our center for the first time. On the chest radiograph, the patient presented dextrocardia, hypoplasia of the right lung, and a tubular image in a vertical position that emptied at the level of the inferomedial portion of the cardiac silhouette, a finding indicative of scimitar syndrome (Figure 1, arrows). Cardiac magnetic resonance confirmed the diagnosis of partial anomalous pulmonary venous return and identified the right pulmonary venous drainage to a collector that emptied in the right atrium (RA) (Figures 2 and 3, arrows). Drainage of the left superior pulmonary veins (LSPV) and left inferior pulmonary veins (LIPV) to the left atrium (LA) was normal (Figure 2). In addition, a type II atrial septal defect was identified. Cardiac catheterization identified an oxymetric inconsistency in the RA (oxygen saturation: 83% in the superior vena cava and 88% in the right atrium). The ratio pulmonary flow/systemic flow was 1.7 and there was no pulmonary hypertension. Initially, conservative treatment with close follow-up of the patient was decided.

Figure 1.

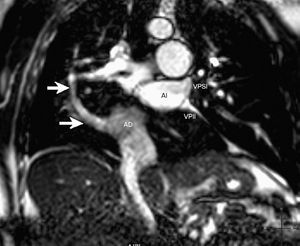
Figure 2.

Figure 3.
Scimitar syndrome accounts for 3%-5% of cases of partial anomalous venous return. The condition is characterized by a combination of anomalous right pulmonary return in the inferior vena cava or right atrium, right pulmonary hypoplasia, and dextrocardia. The prognosis of these patients is usually good with conservative treatment, although surgical treatment is considered in symptomatic patients and those with other associated cardiac anomalies.