A 47-year-old man was admitted to hospital with a 3-month history of exertional dyspnea and lower extremity edema. Computed tomography revealed cardiomegaly and multicompartmental mediastinal adenopathy. The echocardiogram showed left and right ventricular dilation with severely depressed contractility. Magnetic resonance imaging revealed a dilated, nonhypertrophic left ventricle with severe systolic dysfunction (ejection fraction of 16%) and diffuse hypokinesis with no segmental alterations. Following gadolinium administration, there was no sign of late enhancement that could suggest areas of myocardial fibrosis or necrosis. In the assessment of dilated cardiomyopathy of unknown etiology, it is necessary to rule out a toxic origin and perform coronary angiography to exclude important stenotic arterial lesions.
The presence of adenopathy required exclusion of a lymphoproliferative process through mediastinoscopy. The histological examination of the findings revealed nonnecrotizing granulomatous lymphadenitis, indicative of sarcoidosis.
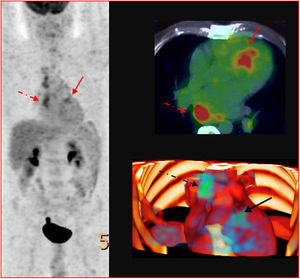
We performed 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT), which showed metabolic activity in the mediastinal lymph nodes (Figure, broken arrow) and a hypermetabolic focus in left ventricular segment 2 (Figure, unbroken arrow).

The Japanese Ministry of Health and Welfare has established 2 diagnostic scenarios in cardiac sarcoidosis: biopsy, an aggressive procedure with limited sensitivity (20%-50%), or one or more diagnostic criteria (echocardiogram, cardiac magnetic resonance imaging, or 18F-FDG PET/CT).
Given the results of mediastinoscopy and 18F-FDG PET/CT, we considered that the both the mediastinal adenopathy and the myocardial involvement had their origin in the sarcoidosis. The decision was made to initiate immunosuppressive therapy, avoiding the performance of myocardial biopsy. The patient has responded favorably to treatment, with no evidence of cardiac complications.