We read with interest the letter by Montero-Cabezas et al1 concerning an uncommon electrocardiographic pattern described as “occlusion of left anterior descending artery without ST-segment elevation”, which in our opinion, and in agreement with the authors of that letter, is highly important since it often leads to a diagnosis of non–ST-segment elevation acute coronary syndrome (NSTEACS) and treatment (reperfusion therapy) is considerably delayed. We would like to make the following comments.
In our experience, this pattern corresponds to a point in the development of ST-segment elevation acute coronary syndrome (STEACS) at which there is a critical subocclusion of the artery, which is ultimately occluded, producing ST-segment elevation. As the latter may not appear until the last moment, its detection requires the performance of numerous serial electrocardiograms. One case that supports this assertion is the sequence of changes observed nearly 70 years ago by Dressler and Roesler,2 and the possibility of detection of a “De Winter pattern”3 following thrombolytic therapy in STEACS (Figure).

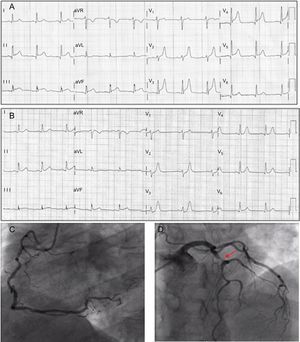
A: Electrocardiographic pattern of ST-segment elevation acute coronary syndrome due to occlusion of left anterior descending artery with a notable apical recurrent segment. B: “De Winter pattern” in anterior leads following thrombolytic therapy. C: Right coronary artery without significant lesions. D: Critical subocclusion of left anterior descending artery.
The authors mention that the exact electrophysiological mechanisms involved in the electrocardiographic changes are unknown. In this respect, we wish to point out that the presence of tall, symmetrical T waves associated with J-point depression can persist for hours, often due to aggressive antiplatelet/antithrombotic therapy that impedes the progression to ST elevation. In the absence of this treatment, as can be seen in the original 1947 article by Dressler and Roesler,2 the result would have been a tracing characteristic of Q-wave myocardial infarction with ST elevation. According to Birnbaum et al,4 this would correspond to grade 1 ischemia, and collateral circulation or ischemic preconditioning is frequently present (Gorgels5). The most logical explanation for the tall, peaked T wave and moderate ST-segment depression is the occurrence of a delay in repolarization in the subendocardial region, with a change in the transmembrane action potential shape (slow rise time and long duration). The addition of this small change to the transmembrane action potential of the subepicardium explains the J-point depression and the tall T wave in the electrocardiographic tracing.
The “De Winter pattern” is just another of the confounding patterns observed throughout the development of STEACS with which health care professionals treating these patients should be familiar, because a delay in the diagnosis leads to large myocardial infarctions.