We present the case of a 76-year-old male patient who was seen at our center for anginal chest pain that had started 24hours earlier. The electrocardiogram at admission showed pathological inferolateral Q-waves with ST segment elevation in the inferolateral leads. An emergency coronary angiography was performed, which showed occlusion of the proximal circumflex artery and insignificant abnormalities in the other arteries (Figures 1A and B). In this situation, we decided to treat the artery that was causing the infarction, implanting a Multilink 8 3/23mm stent (Abbott Vascular; Santa Clara, California, United States), with optimal angiographic result (Figure 1C). In the following 24hours the patient suffered two episodes of acute pulmonary edema, which were controlled with diuretic and vasodilator treatment, with no need for amines or balloon counterpulsation. Afterwards, the patient had residual pulmonary congestion. A transthoracic echocardiogram showed severe mitral regurgitation (MR) due to restriction of the posterior leaflet related to an ischemic condition of the posteromedial papillary muscle (Figure 1D). Twelve hours after this event, the patient suffered acute stroke in the territory of the left middle cerebral artery, from which he recovered completely within hours. With the aim of correcting the valve disorder, we discussed the case with the surgeons, who decided that the risk of surgery would be too high (Society of Thoracic Surgeons [STS] score: mortality, 6.7%; logistic EuroScore, 29.1%).
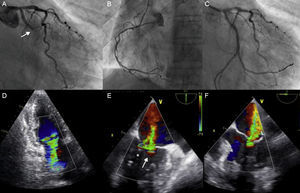
. B: The right coronary artery did not show significant stenosis. C: Angiographic result following percutaneous treatment of the artery causing infarction. D: Transthoracic echocardiography showing severe mitral regurgitation. E and F: Transesophageal echocardiogram showing severe mitral regurgitation with predominant central regurgitation (arrow), although with a certain degree of medial involvement (asterisk).")
A: Coronary angiography showing the thrombotic occlusion of the circumflex artery (arrow). B: The right coronary artery did not show significant stenosis. C: Angiographic result following percutaneous treatment of the artery causing infarction. D: Transthoracic echocardiography showing severe mitral regurgitation. E and F: Transesophageal echocardiogram showing severe mitral regurgitation with predominant central regurgitation (arrow), although with a certain degree of medial involvement (asterisk).
Due to the improbability of the patient recovering well if the valve disorder was not corrected, we opted for mitral repair with the MitraClip® system (Abbott Vascular). A transesophageal echocardiography was performed, which showed severe MR with regurgitation in the A2-P2 scallops, although with a certain degree of medial involvement (A3-P3) (Figures 1E and F).
The procedure was performed under general anesthesia and under transesophageal echocardiographic guidance. After grasping both leaflets in the A2-P2 position, regurgitation reduced noticeably, although residual moderate MR persisted in the area lateral to the implanted clip (Figure 2A). We therefore implanted another clip, lateral to the former, managing to reduce MR to < 1/4 (Figures 2B and C).

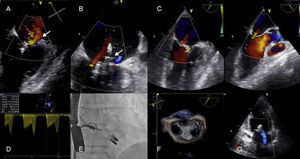
A: Result following implantation of the first clip. Moderate residual regurgitation is visible, lateral to the implanted clip. B: Result following implantation of the second clip laterally to the first with reduction of MR from severe to mild. C: X-plane showing mild residual regurgitation after treatment with the two clips. D: Medium transmitral gradient following implantation of the devices. The final gradient is < 5mmHg. E: Fluoroscopic image showing the position of both clips. F: 3-dimensional image showing the “double orifice” after mitral repair. G: Follow-up echocardiography showing mild residual regurgitation.
The course was favorable thereafter, with complete disappearance of symptoms and signs of heart failure. A check-up echocardiogram 4 days later showed mild residual MR (Figure 2G). The patient was discharged from hospital and is currently New York Heart Association class I.
Acute MR in a context of infarction with ST elevation due to papillary muscle dysfunction is considered to be a mechanical complication that usually causes the patient's clinical worsening and leads to pulmonary edema and sometimes cardiogenic shock. In this scenario, mitral surgery is considered to be the treatment of choice. However, this kind of surgery is associated with high mortality1 due to the high risk profile of patients, which is why surgeons sometimes decide against it. This is the context in which transcatheter valvular treatment techniques are gaining respect. The MitraClip® is the only device for treating mitral valves that is widely used on a clinical level, and mainly in Europe. Recent studies show that the use of this device is safe and effective, achieving functional class improvement in 80% of cases and a persistent reduction in MR after one year.2–4 However, the information on treating patients with acute MR is scarce.5 As this is a phenomenon of recent onset and of functional etiology, the leaflets present characteristics of abundant tissue and coaptation surface that are usually suitable for implanting a clip. Correction of MR leads to rapid clinical recovery, as the volumetric overload is effectively corrected, but there are few data on the effect of the clip on ventricular remodeling after infarction. More studies, with appropriate imaging follow-up, are therefore necessary.
This case shows that mitral repair with the MitraClip® device is a safe and effective technique for correcting acute MR following infarction in patients at high surgical risk. This fact could extend the indications for use of the device to include this patient population.