To the Editor,
We present the case of a male patient of 77 years who was referred with abdominal pain and fever lasting 3 days. With the diagnosis of cholangitis, parenteral treatment with ciprofloxacin 400 mg bid was started. After 48 h of antibiotic treatment, it was decided to perform an endoscopic retrograde cholangio-pancreatography, ERCP. On arriving at the endoscopy suite, the patient had syncope without prodrome, with rapid recovery. He was admitted to the intensive care unit, and repeatedly had wide polymorphic QRS tachycardia with regular rhythm, together with loss of consciousness and tonic-clonic movements that required electrical cardioversion on several occasions.
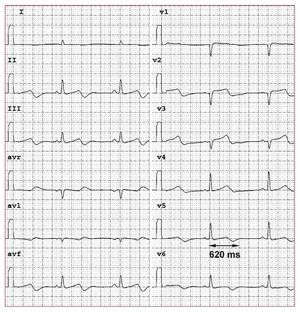
With the diagnosis of polymorphic ventricular tachycardia and long QT (QTc, 596 ms) (Figure 1), it was decided to implant a temporary pacemaker electrode with stimulation in the right ventricular apex at frequencies below 80 beats/min. After this, there were no new clinical or electrocardiographic episodes. After 72 h without ciprofloxacin, the temporary stimulation was withdrawn and the disappearance of changes in cardiac repolarisation was noted.

Figure 1. Electrocardiogram after administration of ciprofloxacin with QT of 620 ms and QTc of 560ms: diffuse changes in cardiac repolarisation.
Values of potassium and magnesium were always within normal limits. The only unusual fact was that the echocardiogram showed a slight hypertrophy of the interventricular septum (12 mm in apical and middle segments).
A study of myocardial perfusion at discharge showed no ischaemia or fixed defects and during monitoring the patient suffered no further cardiovascular symptoms.
This was a case of a patient with cardiogenic syncope in relation with several episodes of polymorphic ventricular tachycardia and torsades de pointes (TdP). The prolongation of cardiac repolarisation in the ECG expressed by an increased QT interval is associated with an increased incidence of complex ventricular arrhythmias and sudden death.1
Numerous non cardiovascular drugs are associated with the prolongation of repolarisation. However, the group of quinolones and especially ciprofloxacin (an antibiotic widely used in our environment) are not seen in groups at high risk.2,3 In fact, ciprofloxacin is the quinolone less related to TdP when compared with levofloxacin or others.
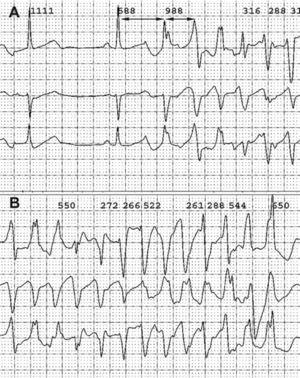
In the ECG in cases of long QT, TdP is initiated by a ventricular extrasystole coinciding with the peak of the T wave of the preceding beat (Figure 2). This extrasystole is generated spontaneously in Purkinje tissue by a phenomenon triggered by early afterpotentials, secondary to a longer than usual repolarisation.

Figure 2. A: plot showing non-sustained polymorphic ventricular tachycardia, with the onset preceded by long-short cycle of premature ventricular contraction (black arrows). B: plot showing syncope with polymorphic ventricular tachycardia: torsades de pointes.
Isoproterenol has been considered as an initial therapy against such arrhythmias, but the best method of preventing further suppression of TdP by suppressing the ectopic activity is the controlled increase in heart rate by external pacing, until the pharmacological effect causing it has disappeared,4 as happened with our patient after 72 h.
One point of contention is whether this effect on repolarisation is only secondary to the drug or part of a genetic predisposition with "silent" defects in the different myocardial ion channels. To investigate this, diagnostic strategies have been proposed, after the acute picture, such as pharmacological (adrenaline) or genetic studies to diagnose abnormalities of intermittent or hidden repolarisation.5
The mechanisms by which quinolones induce QT prolongation are not clear: different authors have found abnormalities in the IKr type potassium channels expressed by the prolongation of the action potential and dispersion of the repolarisation.6
Although the phenomenon described here is unusual, it is important to optimise care in clinical practice with the use of ciprofloxacin, especially at high doses and in patients predisposed to QT prolongation, such as those treated with non-potassium-sparing diuretics or with significant baseline bradycardia.